What does the historical record reveal about how diabetes mellitus was first recognized and understood in ancient Indian and Greek medical traditions, and why did these early physicians associate it with sweetness and excessive urination?
Diabetes mellitus is one of the oldest documented metabolic disorders in medical history. Unlike many conditions that were recognized only after the development of modern science, diabetes mellitus was described thousands of years ago, particularly in ancient Indian medical literature. In Ayurveda, the condition was known as madhumeha, a term that translates to “honey urine.” Ancient physicians observed that the urine of some individuals attracted insects, indicating the presence of sugar long before chemical testing methods were invented. This observation reflects a sophisticated level of clinical awareness rooted in careful sensory examination.
The ancient physician Sushruta, believed to have lived around 1000 B.C., provided one of the earliest meaningful descriptions of diabetes mellitus. He noted that certain individuals experienced excessive thirst, frequent urination, gradual emaciation, and persistent fatigue. Although these healers did not know the biochemical role of insulin, they clearly recognized that something in the body’s regulation of nutrition and energy had gone awry. These early physicians also differentiated between diabetes that appeared in the young and the old, which aligns remarkably well with the modern distinction between type 1 and type 2 diabetes mellitus.
The word diabetes itself comes from the Greek word diabainein, meaning “to pass through,” a reference to the excessive urination that characterizes both main conditions historically labeled as diabetes. The term mellitus, which means “sweetened with honey,” was added later by physicians who observed the sweet taste of the urine, marking the condition as distinct from forms of diabetes where the urine was not sweet. This historical context is key to understanding why two very different disorders, diabetes mellitus and diabetes insipidus, ended up sharing the word “diabetes” while being fundamentally unrelated in cause.
What role does insulin play in converting glucose into energy, and how does the failure of insulin production or utilization lead to the hallmark symptoms and long-term complications of diabetes mellitus?
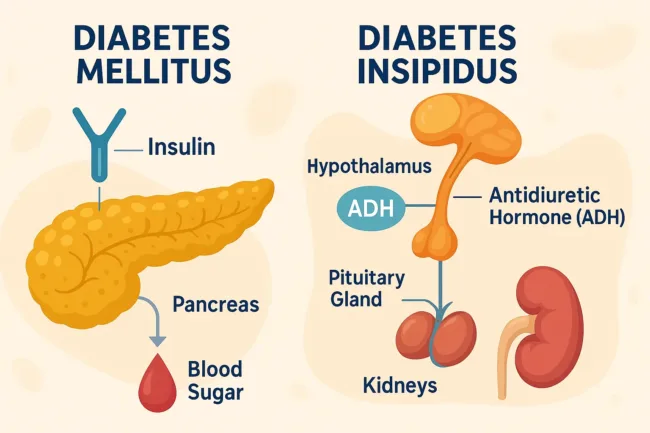
Glucose is one of the body’s primary sources of fuel. After food is consumed, carbohydrates are broken down into glucose, which enters the bloodstream. To use glucose, the cells require the hormone insulin, which is produced by the pancreas, a gland located close to the stomach. Insulin acts as a key that unlocks cells, allowing glucose to move from the bloodstream into the tissues where it can be used for energy production.
When the pancreas does not produce insulin, does not produce enough insulin, or when the cells stop responding effectively to insulin, glucose remains in the bloodstream. This leads to hyperglycemia, or high blood sugar. When blood glucose levels exceed the capacity of the kidneys to reabsorb it, glucose spills into the urine. This phenomenon is called glycosuria, and it contributes to increased urination and dehydration because sugar draws water with it as it exits the body.

Over time, uncontrolled high blood sugar damages small blood vessels throughout the body. The eyes may develop early cataracts or diabetic retinopathy, which can lead to blindness. The kidneys may progressively lose function due to diabetic nephropathy. Nerve fibers can be damaged, leading to pain, numbness, or loss of sensation in the hands and feet. Damage to the heart and blood vessels increases the likelihood of cardiovascular disease. These complications highlight why maintaining blood sugar control is central to managing diabetes mellitus and preventing long-term damage.
What internal hormonal imbalances and cellular responses contribute to the different forms of diabetes mellitus, and why is it considered a group of related disorders rather than a single disease?
Diabetes mellitus is not a single condition but a family of disorders that share the common feature of elevated blood sugar. In some individuals, the pancreas produces little or no insulin, which is characteristic of type 1 diabetes mellitus. In others, the pancreas produces insulin, but the body’s cells do not respond to it effectively. This condition, called insulin resistance, is central to type 2 diabetes mellitus, the most common form worldwide.
The situation becomes more complex when considering the roles of other hormones. The thyroid gland, adrenal glands, pituitary gland, and pancreas all secrete hormones that influence how insulin functions. For example, in Cushing’s syndrome, the body produces excess adrenal hormones that raise blood sugar levels and can produce symptoms similar to diabetes mellitus. Hormones such as glucagon produced in the pancreas act as natural antagonists to insulin, raising blood sugar when needed, but may worsen hyperglycemia when present in excess. Some medications, liver disorders, or systemic diseases can also decrease the effectiveness of insulin or increase the body’s need for it.
This hormonal complexity helps explain why some individuals require daily insulin injections even though their pancreas still produces insulin. In these cases, the issue is not production but utilization. Recognizing diabetes mellitus as a group of metabolic conditions rather than a single disorder allows health professionals to provide more precise and personalized treatment.
What causes diabetes insipidus, and how does impaired secretion or kidney response to antidiuretic hormone lead to excessive urination without affecting blood sugar levels?
Diabetes insipidus is entirely different from diabetes mellitus, despite sharing the symptom of excessive urination. In diabetes insipidus, the problem is not related to blood sugar but to water balance in the body. The hormone responsible for regulating water retention is antidiuretic hormone (ADH), also known as vasopressin. ADH is produced in the hypothalamus and stored in the pituitary gland. When ADH is released, it signals the kidneys to reabsorb water, reducing urine output and helping maintain hydration.
If the hypothalamus does not produce enough ADH or if the pituitary gland fails to release it, the kidneys cannot conserve water, resulting in production of large volumes of dilute urine. Similarly, if the kidneys are unable to respond to ADH, the result is the same. Unlike diabetes mellitus, the urine in diabetes insipidus does not contain sugar, and blood glucose levels remain normal. Individuals with diabetes insipidus may drink large quantities of water to compensate for what is lost, illustrating how profoundly the body depends on hormonal control of hydration.
Treatment for diabetes insipidus focuses on replacing ADH or improving kidney response to it. This may be achieved through medications delivered as nasal sprays, oral tablets, or injections. As long as the condition is recognized and managed, individuals can maintain fluid balance effectively.
Why is distinguishing between diabetes mellitus and diabetes insipidus essential for clinical understanding and public awareness, and how does this knowledge influence modern health care and disease management?
The shared name often leads to misunderstanding, yet the two conditions affect completely different systems, involve different hormones, and require different treatments. Diabetes mellitus involves insulin and blood sugar regulation and can lead to widespread tissue damage if untreated. Diabetes insipidus involves water regulation and the action of ADH. Understanding the difference ensures accurate diagnosis, prevents misinformation, and supports effective treatment choices.
As global rates of diabetes mellitus rise due to lifestyle changes, urbanization, dietary patterns, and longer life expectancy, awareness of metabolic health has become increasingly important. Meanwhile, diabetes insipidus remains relatively rare but requires clear understanding to prevent dangerous dehydration.
Recognizing how these conditions were identified historically also reminds us that careful clinical observation has always been a cornerstone of medical practice. Ancient medical traditions laid the groundwork for modern endocrinology, and today’s treatment strategies continue to build upon that foundation with advanced research, improved therapies, and personalized care approaches.
Discover more from Business-News-Today.com
Subscribe to get the latest posts sent to your email.