


Lumosa Therapeutics Co., Ltd. (6535.TWO) has reported positive Phase 2 clinical data for its investigational stroke therapy LT3001, showing statistically meaningful functional improvements in patients with disabling acute ischemic stroke who are often ineligible for standard reperfusion therapies. The results, presented at the International Stroke Conference, position LT3001 as a potential late-window intervention in a therapeutic area where decades of neuroprotection efforts have failed to translate into approved drugs.
The immediate strategic relevance is not simply the reported efficacy signal, but the patient population targeted. Lumosa Therapeutics Co., Ltd. is explicitly focusing on patients who fall outside intravenous thrombolysis or endovascular thrombectomy eligibility, a group that represents a large share of real-world stroke admissions and remains poorly served by existing standards of care.
Why LT3001’s dual mechanism could matter in acute ischemic stroke where single-pathway drugs have failed
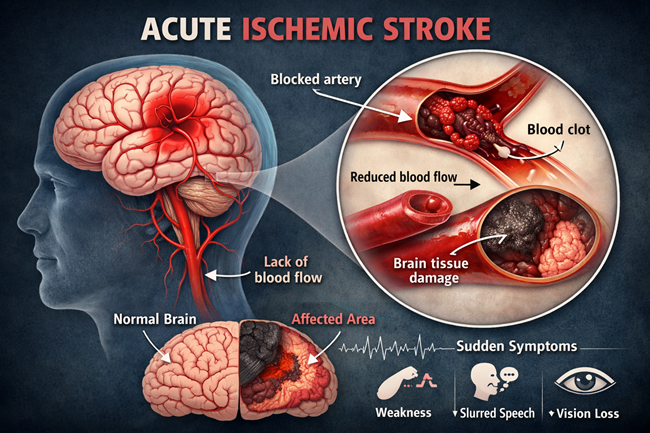
LT3001, also known as odatroltide, is positioned as a dual-functional therapy combining enhancement of endogenous fibrinolysis with direct neuroprotection through free radical scavenging. This approach is notable because most historical failures in stroke drug development have focused on single mechanisms, either clot dissolution or neuronal protection, without addressing the broader ischemic cascade.
In the China-based LT3001-202 trial, moderate acute ischemic stroke patients with disabling symptoms demonstrated absolute improvements of 8 percent in modified Rankin Scale scores of 0–1 and 13 percent in scores of 0–2 compared with placebo. These endpoints are clinically meaningful because they correlate with independence rather than marginal neurological change. In stroke trials, even single-digit percentage gains at these thresholds are often viewed as commercially and clinically relevant if reproducible.
The mechanism also appears to support use beyond the conventional thrombolytic time window. Patients were treated up to 24 hours after symptom onset, a timeframe that reflects real-world hospital presentation patterns but sits outside the comfort zone of most approved pharmacologic interventions.

What subgroup data from large artery atherosclerosis and imaging-selected patients signal for Phase 3 design
One of the more strategically important elements of the Phase 2 data lies in subgroup performance. In the LT3001-202 study, patients with large artery atherosclerosis showed an 11 percent improvement in modified Rankin Scale 0–2 outcomes and a 9 percent gain in 0–1 outcomes versus placebo. These patients often present complex clot biology and limited response to standard thrombolysis, making them a challenging but commercially relevant segment.
The complementary LT3001-205 study, conducted across the United States, Europe, and Taiwan, reinforced these signals using imaging-assisted patient selection. Although smaller in size, the trial showed that mismatch-positive patients achieved a 10 percent absolute improvement in modified Rankin Scale 0–2 outcomes. Among patients with disabling features, 27 percent achieved modified Rankin Scale 0–1 outcomes on LT3001 compared with 17 percent on placebo.
For Lumosa Therapeutics Co., Ltd., this consistency across geography and selection strategy strengthens the argument that Phase 3 should incorporate imaging-based enrichment while retaining broad eligibility. From a regulatory and payer perspective, that balance may prove critical.
How safety and dosing data affect regulatory credibility in a hemorrhage-sensitive indication
Safety remains the Achilles’ heel of stroke drug development, particularly the risk of symptomatic intracranial hemorrhage. According to investigators, LT3001 did not increase symptomatic intracranial hemorrhage rates despite multi-dose administration over three days. That detail matters because many neuroprotective candidates have stumbled on bleeding risk or off-target toxicity when scaled beyond single doses.
The absence of a hemorrhagic penalty supports the company’s argument that LT3001 could be layered onto existing care pathways without materially increasing procedural risk. For regulators such as the U.S. Food and Drug Administration, safety consistency will likely carry as much weight as efficacy magnitude when reviewing Phase 3 protocols.
Why the unmet need narrative remains compelling despite decades of failed stroke drugs
Acute ischemic stroke remains one of the most frustrating therapeutic areas in modern medicine. Despite extensive preclinical success, no neuroprotective drug has gained regulatory approval in the United States. The World Health Organization continues to rank stroke among the leading causes of death and disability globally, with ischemic events accounting for the majority of cases.
Lumosa Therapeutics Co., Ltd. is explicitly framing LT3001 as a response to this systemic failure, rather than a marginal upgrade to existing thrombolytic strategies. By targeting patients who cannot receive intravenous thrombolysis or endovascular thrombectomy, the company is aligning clinical development with the largest untreated segment of the market, rather than competing head-to-head with entrenched standards.
What FDA feedback and global Phase 3 plans suggest about execution risk and timelines
Lumosa Therapeutics Co., Ltd. has confirmed that it has received feedback from the U.S. Food and Drug Administration regarding Phase 3 development plans. While details remain undisclosed, the acknowledgment signals regulatory engagement rather than exploratory dialogue. For investors and partners, that distinction reduces perceived development risk, even as Phase 3 scale and cost remain significant hurdles.
Global Phase 3 execution will require careful site selection, imaging standardisation, and endpoint discipline. Stroke trials are operationally complex, and variability in care standards across regions can dilute outcomes. The company’s ability to translate Phase 2 signals into a registrational study will hinge on operational rigor as much as scientific rationale.
How investors and institutional markets are likely to interpret Lumosa Therapeutics Co., Ltd.’s Phase 2 LT3001 stroke data
As a publicly traded Taiwanese biotechnology company, Lumosa Therapeutics Co., Ltd. operates outside the core U.S. biotech spotlight, but positive late-stage neurological data can rapidly change visibility. Neuroprotection remains a high-risk, high-reward category, and investors are likely to view the LT3001 data as an option-value inflection rather than a near-term revenue catalyst.
Market sentiment is likely to remain cautious but constructive. The absence of safety red flags and the focus on underserved patients support a differentiated narrative, while the historical failure rate in stroke drug development tempers enthusiasm. Institutional interest will likely depend on Phase 3 design transparency, partnering signals, and clarity on funding strategy.
What LT3001’s progress signals about the future direction of acute ischemic stroke drug development
If LT3001 advances successfully into Phase 3, it could influence broader industry strategy by validating combination mechanisms and extended treatment windows. For competitors and larger pharmaceutical companies, the data reinforce the idea that incremental tweaks to thrombolysis alone may not be sufficient to move outcomes meaningfully.
The program also highlights the renewed importance of imaging-guided patient selection, not as a niche strategy but as a core component of stroke drug development. If regulators accept this framework, it may reshape how future candidates are designed and evaluated.
Key takeaways on what Lumosa Therapeutics’s LT3001 data mean for the company, competitors, and the stroke drug market
- LT3001 shows functional outcome improvements in disabling acute ischemic stroke patients who lack standard treatment options
- Dual-mechanism design addresses both clot biology and neuronal injury, differentiating LT3001 from historical failures
- Consistent signals across two Phase 2 trials strengthen the rationale for global Phase 3 development
- Safety data without increased hemorrhage risk support regulatory credibility in a high-risk indication
- Imaging-assisted patient selection may become central to future stroke drug trials if validated in Phase 3
- The program targets a large, underserved patient population with meaningful commercial potential
- Investor sentiment is likely to view the asset as an option-value inflection rather than a near-term catalyst
- Successful Phase 3 execution could reposition neuroprotection as a viable commercial strategy after decades of disappointment
Discover more from Business-News-Today.com
Subscribe to get the latest posts sent to your email.

